
Synthetic melatonin is a dietary supplement. The FDA does not regulate supplements. Therefore, melatonin is not officially FDA-approved for any indication. However, there are several melatonin receptor agonists on the market, such as ramelteon and tasimelteon, which are FDA-approved for the treatment of insomnia.
Non-FDA Approved Indications for Melatonin
Sleep
Despite the lack of FDA approval, melatonin is considered first-line pharmacologic therapy for the treatment of insomnia by the American Academy of Family Physicians (AAFP). It is relatively safe with a low risk of side effects.
Studies on the efficacy of melatonin supplementation for the treatment of insomnia have varied, but one metanalysis by Ferracioli-Oda showed that subjects taking melatonin fell asleep an average of 7 minutes faster, stayed asleep about 8 minutes longer, and reported better sleep quality than subjects receiving a placebo. Doses used, results, and study quality varied considerably between trials.
Melatonin has been studied and recommended primarily for the treatment of the following:
- Primary insomnia (insomnia not due to some secondary cause)
- Age-related insomnia
- Jet lag
- Shift work
- Post-traumatic brain injury
- Neurodegenerative disorders
Other Ongoing Research
Although there are no formal recommendations at this time, research is also being conducted on the role of melatonin treatment for other conditions, such as:
- Cancer
- Metabolic disorders
- Cardiovascular disorders
- Gastrointestinal (GI) conditions
- Neurodegenerative disorders
- Mental disorders
- Pain syndromes
- Reproductive dysfunctions
Go to:
Mechanism of Action
Synthesis of Endogenous Melatonin
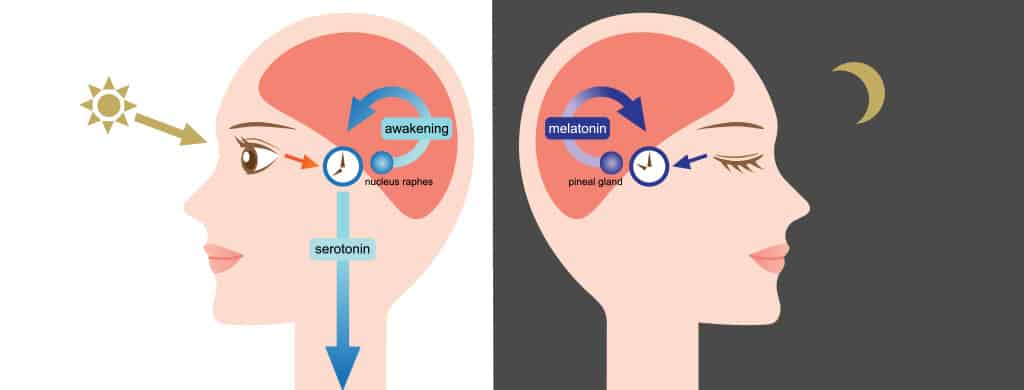
Endogenous melatonin is a hormone produced naturally by the body, synthesized and secreted primarily in the pineal gland. Melatonin production begins with tryptophan, which is converted via a several-step pathway to serotonin in other parts of the brain. Some of the serotonin produced makes its way to the pineal gland, where it is converted to melatonin in a cyclic, light-dependent process.[12]
The conversion of serotonin to melatonin is controlled by the suprachiasmatic nucleus (SCN) of the hypothalamus, the coordinator of the circadian rhythms of the body. Information about low light to dark condition travels from the retina along the retinohypothalamic tract to the SCN. The SCN, in turn, sends signals through the sympathetic nervous system to the superior cervical ganglia, which innervates the pineal gland.
Sympathetic stimulation of the pineal gland upregulates the production of the enzyme arylalkylamine N-acetyltransferase (AA-NAT). AA-NAT functions to convert serotonin to N-acetyl-serotonin, the rate-limiting step in melatonin formation. This intermediate is then converted to melatonin. Studies have shown that bilateral surgical removal of the superior cervical ganglia or SCN in rats stops the activation of AA-NAT and eliminates the rhythmic pattern of melatonin secretion, which disrupts the sleep-wake cycle.[13][14][15]
Functions of Endogenous Melatonin
Sleep
The best-known purpose of melatonin is its role in the promotion of sleep. Melatonin is released from the pineal gland into the third ventricle, and from there into circulation. Melatonin is involved in the regulation of the body’s sleep-wake cycles through its interactions with the suprachiasmatic nucleus of the hypothalamus and the retina, both promoting sleep and inhibiting wake-promoting signals via interactions with its MT1 and MT2 receptors.
Other Biological Functions of Melatonin Under Study:
Cancer suppression: Activation of tumor suppressor genes such as p53, oncostatic activity, modulation of estrogen and androgens, immunomodulation, increased cytokine production, and others
Bone deposition: MT2 receptors are found on osteoblasts, suggesting a role for melatonin in regulating their function
Metabolic disorders: Anti-oxidative effects, anti-inflammatory effects, regulation of lipid and glucose metabolism
Cardiovascular diseases: Anti-hypertensive effects
GI conditions: Anti-oxidative effects, anti-inflammatory effects
Neurodegenerative disorders: Activation of mitochondrial cell survival pathways that may protect against neurodegeneration caused by mitochondrial dysfunction. Regulation of apoptosis. Prevention of vasoconstriction of cerebral arteries
Mental disorders: Anxiolytic; the melatonin receptor agonist agomelatine is approved for the treatment of depression in Europe.
Pain syndromes: Anti-nociceptive, anti-inflammatory, and analgesic effects
Reproductive functions: Involvement in several pathways resulting in a reduced risk of complications, gonadotropic secretion, and higher rates of mature oocytes and quality embryos[19]
Go to:
Administration
Melatonin Content of Supplements
Supplements are generally presumed safe and are not regulated by the FDA. However, this can lead to concerns about the actual concentrations of supplements, including melatonin. One study analyzed 31 melatonin supplements and found that actual melatonin content ranged from -83% to +478% of the labeled content. Variable tablet content can make accurate dosing difficult and may be responsible for some of the wide ranges of efficacy reported in various trials. One way to assure correct dosing is to look for supplements with approval from the United States Pharmacopeia, an independent non-profit organization. Searching for supplements marked “USP verified” can help assure the quality and dosing of supplements.
Routes of Administration
- Oral tablet
- Oral liquid
- Rectal suppository
- Transdermal patch
Formulations
- Immediate-release
- Extended-release
- Combined immediate and extended-release
Dosing
As the FDA does not regulate melatonin as a drug, effective dosing is not well-defined. Dosing used in studies varied from 0.1 to 10 mg, administered up to two hours before bedtime.
Maximum Dosage
Not defined in trials
Elimination Half-Life
One to 2 hours, depending on the formulation
Bioavailability
Highly variable, 1% to 74%, likely dependent on formulation and dose
Metabolism
Ninety percent of melatonin is metabolized in the liver primarily by the enzyme CYP1A2. It is metabolized by hydroxylation to 6-Hydroxymelatonin, conjugated to sulfuric or glucuronic acid, and excreted in the urine. A smaller amount is excreted in feces.
Go to:
Adverse Effects
Melatonin is relatively non-toxic, although some mild side-effects have been reported with higher doses and extended-release formulations, including:
- Drowsiness
- Daytime sleepiness
- Headaches
- Nausea
No evidence suggests that people develop tolerance to melatonin.
Go to:
Contraindications
Pregnancy and Breastfeeding
Melatonin is not recommended for pregnant or breastfeeding women due to insufficient evidence of safety although this is under study.[19]
Renal Dosing
Caution is advised for dialysis patients due to the risk of increased adverse effects due to the inability to adequately clear melatonin.
Hepatic Dosing
Caution is advised for patients with impaired liver functioning due to decreased ability to metabolize melatonin. Further studies into possible effects versus benefits are pending.
